


1. Background
For over four decades, nasal continuous positive airway pressure (nCPAP) has been considered the standard care for managing respiratory distress syndrome (RDS). Despite its physiological and clinical benefits, the failure rate of nCPAP in extremely preterm neonates during the first week of life is approximately 50%. This failure is associated with a significant increase in adverse outcomes, including chronic lung disease, air leak syndromes, intracranial hemorrhage, and mortality (1-6). In the past two decades, the adoption of non-invasive cycled-PAP approaches has grown steadily in neonatal intensive care units (NICUs) aimed at improving the quality of respiratory management interventions. Non-invasive positive pressure ventilation (NIPPV) has emerged as a primary mode in NICU settings, particularly when implemented within 2 hours of birth in an infant with respiratory distress. However, the application of NIPPV in RDS remains variable; for instance, in the UK, its use as a primary mode ranges from 48% in England to 61% in Ireland (7-9).
The physiological effects associated with NIPPV include improved end-expiratory lung volume through positive end-expiratory pressure (PEEP), which results from increased mean airway pressure (MAP), ultimately contributing to elevated functional residual capacity (FRC) and lung compliance. Additionally, studies indicate that neonates under NIPPV experience lower respiratory rates, reduced respiratory effort, and fewer apneic episodes compared to those under nCPAP. However, much of these benefits were reported when nasal ventilation (NV) or non-invasive ventilation (NIV) was synchronized NIPPV (SNIPPV) using Infrasonics Infant Star ventilators and pneumatic capsules (Graseby), with researchers also noting a reduction in thoraco-abdominal asynchrony (10, 11).
The optimal goal of NIV in clinical settings is to achieve pressure transitions from expiratory positive airway pressure (EPAP) to inspiratory positive airway pressure (IPAP) when the glottis is open. However, since a preterm infant is considered an "exteriorized fetus", they tend to maintain a fetal respiratory pattern, as observed clinically. High thyroarytenoid muscle activity and limited cricothyroid muscle activity cause vocal cords to significantly resist gas flow. Airway obstruction, especially during increased inspiratory gas flow, frequently occurs unless the infant demonstrates regular, spontaneous breathing (in which case the glottis and epiglottis –larynx – keep the airway open). Conversely, spontaneous breathing can lead to pharyngeal collapse, especially in the highly compliant pharynx during inspiration, potentially causing partial or total supraglottic airway obstruction (12).
When NIV is non-synchronized, the application of IPAP during spontaneous breaths, periods of limited laryngeal caliber, or expiration can trigger abnormal stimulation of bronchopulmonary receptors sensitive to mechanical pressure. This stimulation may activate the apneustic center in the pons, leading to glottal closure. Furthermore, studies have shown that increasing IPAP levels (IPAP ≥ 7 cm H2O) to overcome this process or increasing tidal volume can intensify and prolong glottal obstruction. These alterations in glottal muscle activity during NIPPV, when accompanied by recurrent apneas and hypoxia, can lead to the failure of NIV and the need for invasive ventilation (13, 14).
Considering that the larynx can act as a closing valve during NIV, potentially limiting its effectiveness, the development of synchronization techniques in non-invasive cycled positive airway pressure (cycled-PAP) has been investigated over the past decade. Multiple techniques have been employed for this purpose, including:
1. Flow-sensor usage: Detecting inspiratory gas flow to cycle the ventilator using a flow-triggering mechanism.
2. Thoracic impedance monitoring: Detecting resistance changes in electrical current passage through the chest due to liquid-to-gas ratio changes during breathing to manage ventilator cycling.
3. Diaphragmatic electrical activity (NAVA/neurally adjusted ventilator assist): Leveraging electrical activity of the diaphragm, which synchronizes the breathing pattern proportionally to NIV.
It is noteworthy that the Puritan Bennett approach using pneumatic capsules for synchronizing NIV, previously used in Infrasonics Infant Star 950/500 ventilators, has recently gained renewed attention (15, 16).
2. Objectives
The technology for monitoring pressure changes during the respiratory cycle to synchronize NIV has advanced significantly. Even in flow-driven generators such as Medijet (Medin-Hamilton Medical Company, Olching, Germany), despite significant gas leakage inherent to flow drive technology, the application of SNIPPV has been emphasized (17).
While a limited number of studies examine the management of RDS using SNIPPV with pressure-triggered systems, given the technological developments, especially in the past two decades, we decided to investigate RDS management in infants using two approaches — NIPPV and SNIPPV — through a clinical trial utilizing Stephan Company ventilators (Fritz Stephan GmbH, Gackenbach, Germany). These ventilators can monitor pressure in the proximal circuit during NIV and use it for triggering.
3. Methods
3.1. Design and Setting
This study was a randomized controlled trial (RCT) conducted from August 2023 to September 2024 at Shahid Beheshti and Al-Zahra hospitals in Isfahan, Iran. Inclusion criteria comprised neonates with a gestational age of 28 to 32 weeks diagnosed with RDS (based on clinical and radiological signs), who were placed on nCPAP within the first 2 hours of birth and received surfactant during the INSURE process. Exclusion criteria included:
- Neonates with potential chromosomal or genetic abnormalities
- Major congenital malformations
- Contraindications limiting NIV, such as:
(1) Need for midface surgical interventions (involving nose, mouth, or digestive system)
-Evidence of perinatal asphyxia, defined by at least one or two of the following parameters:
(1) Apgar score < 6 at 10 minutes
(2) Requirement for positive pressure ventilation or chest compression with positive pressure ventilation at 10 minutes
(3) Any acute perinatal sentinel event potentially causing hypoxic-ischemic encephalopathy (e.g., placental abruption, umbilical cord prolapse, severe FHR abnormalities)
(4) Umbilical or arterial blood sample pH < 7 or base excess ≤ -16 mmol/L within one hour of birth
This study was registered on the Iranian Registry of Clinical Trials (reference number: IRCT20120728010430N12).
3.2. Patients
Neonates meeting the inclusion criteria were enrolled in the study. Following surfactant administration and stabilization under mechanical ventilation, neonates meeting extubation criteria were weaned from invasive ventilation, transitioned to NIV, and randomly assigned to either of two groups through a computer-generated sequence: NIPPV or SNIPPV. Table 1 presents the demographic characteristics of the participants. Each group required 35 neonates to achieve statistical significance.
| Variables | NIPPV | SNIPPV | P-Value |
|---|---|---|---|
| Sex | 0.811 | ||
| Male | 18 (51.42) | 19 (54.28) | |
| Female | 17 (48.57) | 16 (45.71) | |
| GA (wk) | 29.92 ± 1.60 | 30.04 ± 1.54 | 0.754 |
| Birth weight (g) | 1318.86 ± 456.10 | 1299 ± 414.58 | 0.849 |
| Mothers receiving steroids | 24 (68.57) | 19 (54.28) | 0.220 |
| Route of delivery | 0.474 | ||
| NVD | 13 (37.14) | 16 (45.71) | |
| C/S | 22 (62.85) | 19 (54.28) |
Demographic Characteristics of Newborns in Two Groups a
3.3. Intervention
Neonates were initially supported with nCPAP using a constant flow CPAP system (EasyFlow nCPAP, Fritz Stephan GmbH, Gackenbach, Germany) and a Sophie ventilator (Fritz Stephan GmbH, Gackenbach, Germany). If the neonate required an inspiratory oxygen fraction (FiO2) > 30% to maintain right-hand oxygen saturation levels between 90% - 94% while on continuous distending pressure (CDP) ≥ 6 cm H2O, they were removed from nCPAP, intubated, and transitioned to mechanical ventilation in A/C mode. The parameters of mechanical ventilation included PEEP = 6 - 8 cm H2O, PIP = 15 - 20 cm H2O, and inspiratory time (Ti) = 0.25 - 0.30 seconds. Flow-triggering was adjusted to detect and support at least 80% of the neonate’s spontaneous breaths. A chest X-ray was performed to verify appropriate endotracheal tube placement, and blood gas parameters were stabilized to acceptable levels (pH: 7.25 - 7.35, PCO2: 45 - 55 mmHg, HCO3-: ≥ 16 mmol/L). Then, the neonate received a dose of Beractant (Beraksurf, Tekzima Co, Tehran, Iran) surfactant. All interventions were completed within two hours of birth. If the neonate’s hemodynamics and blood gases were stable, they were deemed ready for extubation. Before extubation, dynamic pressure [PIP - 1/2 (Pplat - PEEP)] was calculated; in order to calculate Pplat (plateau pressure), an inspiratory pause was used. It should be noted that Pplat equals static pressure. Neonates whose parents provided informed consent were then randomly assigned to either of the two study groups (SNIPPV or NIPPV) following extubation (18-20).
For infants in the NIPPV group, the EasyFlow prongs were attached, and NIV parameters, including IPAP = dynamic pressure, EPAP = 5 cm H2O, Ti = 0.45 seconds, and rate = 25 bpm, were defined for the ventilator in IMV respiratory mode. For infants in the SNIPPV group, NIV parameters, including IPAP = dynamic pressure, EPAP = 5 cm H2O, Ti = 0.25 seconds, and pressure trigger = 20% (dynamic pressure), were defined for the ventilator in AC respiratory mode. In cases when an infant's need for inspiratory oxygen fraction remained higher than 40% to maintain oxygen saturation in an acceptable range, Beractant was re-administered 6 hours after the previous surfactant dose, up to a maximum of four doses in the therapeutic course. Capillary blood gas (CBG) measurements were performed before and after administering each surfactant dose and every 12 hours thereafter. Adjustments in respiratory management were made based on CBG results. For infants whose oxygen saturation level, despite surfactant administration, still did not fall within the acceptable range, EPAP was initially increased by 1 - 2 cm H2O, and then FiO2 was increased by 5 - 10% as needed. The weaning process included reducing EPAP and then FiO2, with the infant being separated from respiratory support at EPAP = 4 cm H2O and FiO2 ≤ 25%.
3.4. Criteria for Intubation and Mechanical Ventilation
If any of the following occurred, NIV was discontinued, followed by intubation and invasive mechanical ventilation: Inability to establish acceptable ventilation and respiratory failure (pH < 7.2 & PCO2 > 65 mmHg), more than three apnea episodes per hour requiring stimulation or ventilation with bag and mask, and FiO2 > 75% requirement to maintain oxygen saturation within the 90 - 95% range (21-24).
the results obtained from the characteristics questionnaire, the need for mechanical ventilation within the first 72 hours of life, the number of surfactant doses administered, the duration of non-invasive respiratory support, the incidence of pneumothorax, and the duration of oxygen requirement (requiring oxygen beyond day 28 would lead to a CLD diagnosis for the neonate) were documented. Brain ultrasound was performed on infants on the third, seventh, and fourteenth days after birth to assess IVH and PVL, and then the results were recorded.
3.5. Main Outcome Measures
The primary objective of this research project was to statistically assess and compare the need for mechanical ventilation in the NIPPV and SNIPPV groups within 72 hours following birth.
4. Results
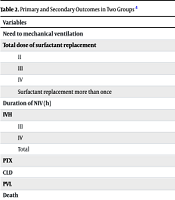
Table 2 outlines the study's objectives. There was no significant difference in the need for mechanical ventilation between the two groups. Similarly, no significant difference was observed in the requirement for surfactant administration beyond the initial dose. The duration of NIV and the incidence of chronic lung disease also did not significantly differ between the two groups. Furthermore, the occurrence of intraventricular hemorrhage (grades III and IV) and periventricular leukomalacia showed no significant differences. Finally, the rates of pneumothorax and mortality did not significantly differ between the two groups.
| Variables | NIPPV | SNIPPV | P-Value |
|---|---|---|---|
| Need to mechanical ventilation | 12 (34.28) | 10 (28.57) | 0.607 |
| Total dose of surfactant replacement | |||
| II | 7 (20) | 5 (14.28) | 0.526 |
| III | 4 (11.42) | 5 (14.28) | 0.721 |
| IV | - | 2 (5.71) | 0.151 |
| Surfactant replacement more than once | - | - | 0.274 |
| Duration of NIV (h) | 35.26 ± 6.56 | 42.17 ± 18.98 | 0.732 |
| IVH | |||
| III | 4 (11.42) | 3 (8.57) | 0.690 |
| IV | 2 (5.71) | 1 (2.85) | 0.555 |
| Total | - | - | 0.495 |
| PTX | 2 (5.71) | 1 (2.85) | 0.555 |
| CLD | 11 (31.42) | 12 (34.28) | 0.799 |
| PVL | 2 (5.71) | 1 (2.85) | 0.555 |
| Death | 11 (31.42) | 6 (17.14) | 0.166 |
Primary and Secondary Outcomes in Two Groups a
5. Discussion
While designing the current study, potential sources of bias were recognized and carefully considered. Firstly, randomization was performed using a computer-generated sequence to minimize selection bias. To address performance and detection bias, all clinical staff involved in patient care and outcome assessment were uniformly trained and adhered to standardized protocols. Furthermore, outcome evaluators were blinded to the assigned intervention groups whenever possible. Attrition bias was minimized by ensuring complete follow-up of all enrolled participants throughout the study period.
In a context similar to that of our research, limited studies have explored synchronization using pressure-level variations during respiratory cycles generated by the patient. For example, in Kugelman's study, which was carried out in 2007 at Los Angeles Children’s Hospital, California, neonates younger than 35 weeks of gestation with RDS were managed in an RCT comparing nCPAP (41 infants) with SNIPPV (43 infants). This study utilized the Newport E100M ventilator, Inca injector, short binasal prong (Covidien), and a pressure trigger for cycling the ventilator. While SNIPPV significantly reduced the need for invasive ventilation and the incidence of chronic lung disease, the researchers were unable to validate or document synchronization during spontaneous breaths (25). Nevertheless, the results of the present study did not show any significant difference in the effectiveness of SNIPPV versus NIPPV in reducing the need for invasive ventilation or the incidence of chronic lung disease.
In another study conducted by Nabeel et al. at Miller University Hospital in Miami, Florida, preterm infants (weighing between 500 g to 1500 g) requiring nCPAP with FiO2 < 50% due to RDS were supported using NI-PSV. This intervention utilized the Sechrist (IV200SAVI) ventilator and Inca injector. The synchronization hardware relied on Respiratory Inductance Plethysmography (RIP), whereby the ventilator trigger was defined as the sum of signals from thoracic and abdominal loops. Additionally, regarding pressure support level, esophageal pressure (PES), which was measured using a balloon connected to a manometer placed in the lower esophagus to reflect pleural pressure, was employed to adjust the proximal pressure line during inspiration to 100% - 150% of PES. This system provides researchers with the ability to determine tidal volumes and minute ventilation at various positions. This study showed that WOB (Work of Breathing) in the NI-PSV intervention was significantly lower than in nCPAP (26).
In a study by Gao et al. in 2010 at the Guangdong Children's Hospital (Guangzhou, China), infants with RDS and a gestational age less than 37 weeks were divided into nCPAP and nSIMV groups after receiving surfactant, with each group consisting of 50 infants. The Comen NV8 ventilator (Shenzhen Comen Medical Instruments Co. Ltd.) was used, employing a pressure trigger for nSIMV. The study revealed that the nSIMV group exhibited significantly lower treatment failure and hypercapnia rates (P < 0.05) (27). Nonetheless, in the current study, the need for MV as calculated did not differ significantly between the SNIPPV and NIPPV groups.
Ding et al. conducted a study across Anhui Medical University Hospital (Hefei, China), Xiangya Hospital of Central South University (Changsha, China), and Jilin University Hospital (Changchun, China) from 2017 to 2018. They grouped preterm neonates with RDS (gestational age < 32 weeks) requiring mechanical ventilation and surfactant therapy shortly after birth into three intervention categories after extubation: The nCPAP, SNIPPV, and a sequential group (alternating between SNIPPV and nCPAP), each consisting of 40 neonates. The Comen NV7 ventilator (Shenzhen Comen Medical Instruments Co. Ltd) was used to conduct this study. No significant differences among the three groups in terms of hospital stay duration or the time required for supplemental oxygen were found in this study (28). The results of Ding et al.’s study were in line with those obtained in the present study.
Considering the primary outcome, this study was unable to demonstrate a statistically significant reduction in the need for invasive mechanical ventilation in the SNIPPV group. This contrasts with earlier findings by Kugelman and Gao, which showed a significant reduction in mechanical ventilation requirements in the SNIPPV group. Additionally, unlike Kugelman's study, which demonstrated significantly reduced chronic lung disease in the SNIPPV group, no significant difference in chronic lung disease was observed in this study.
5.1. Conclusions
Considering the variables, the present study was unable to showcase any potential significant differences between the efficiency of NIPPV and SNIPPV in managing RDS. This study could serve as a basis for larger-scale studies, potentially contributing to the development of this evidence-based therapeutic approach.
5.2. Limitations
One limitation of this study is the small sample size. Advances in pressure sensor sensitivity over the past decade offer hope for improved technical precision in future research.
5.3. What Did We Already Know in This Domain?
Synchronization of respiratory machines during non-invasive respiratory support with the patient's spontaneous breathing is a critical factor in improving respiratory efficiency, avoiding invasive support, and minimizing its associated complications.
5.4. What Did This Study Add to This Knowledge?
Pressure sensors can be effectively utilized to synchronize the performance of respiratory support devices with patients’ spontaneous breathing during non-invasive respiratory therapy, undoubtedly enhancing the quality of this therapeutic approach.
