




1. Background
Vitamin D is an essential micronutrient obtained from the conversion of a provitamin in the skin in the presence of UVB rays from the sun to cholecalciferol, or by consuming food and supplements containing vitamin D through the digestive tract (1). Vitamin D is initially in an inactive form, and to convert into its active form, namely calcitriol, it requires two hydroxylations that are carried out in the liver and kidney (2-4). Calcitriol then binds to vitamin D receptors, which are found throughout the human body and through which it regulates several biological processes (3).
Serum levels of vitamin D in different regions depend on many factors such as season, latitude, cultural factors that lead to reduced exposure to UVB rays, gender, age, skin pigmentation, Body Mass Index, amount of vitamin D in foods, exercise, and physical activity (4). About 1 billion people worldwide are vitamin D deficient. Vitamin D deficiency is more common in Middle Eastern countries and also in people who have more skin melanin or use extensive skin coverage (5, 6).
Constipation is an intestinal dysfunction in which the patient experiences hard, dry, and infrequent stools along with pressure and pain. It is divided into two types: Organic and functional. Functional constipation is multifactorial, and no anatomical, medical, or medicinal cause can be found for it. Functional constipation is more common in children and accounts for about 25% of pediatric gastroenterology visits (7-9). According to the results of a meta-analysis, the prevalence of constipation ranges from 0.5% to 32.2%, with an overall prevalence of 9.5% (10).
Vitamin D has received more attention recently, especially its deficiency, which is associated with many systemic disorders. Apart from its effect on skeletal and extra-skeletal health (11), it has anti-inflammatory effects, modulates the immune system, and also affects gastrointestinal motility (12, 13). The relationship between vitamin D and chronic constipation is probably one of the least studied topics.
2. Objectives
This study aimed to investigate the effect of vitamin D deficiency on the response to constipation treatment in children with functional constipation.
3. Methods
In this cohort study, 62 children aged 1 to 18 years with functional constipation, referred to Ekbatan Hospital in Hamedan, Iran (during 2024), were studied. First, a blood sample from the basilic vein was obtained from all patients, and after centrifugation, the serum level of D(OH)25 was measured by the Enzyme-Linked Fluorescent Assay method (Biomerieux company kit made in France was used).
Based on vitamin D levels, patients were divided into two equal groups: Patients with vitamin D deficiency (study group) and patients without vitamin D deficiency (control group). Then, patients in both groups underwent constipation treatment, and the results of the treatment were evaluated and compared at the end of the second week, the first month, and the second month of treatment.
A vitamin D level equal to or higher than 30 ng/mL was considered normal. Treatment of functional constipation included dietary changes and consumption of Pidrolox powder without electrolytes (manufactured by Sepidage Company) with a dose of 0.7 g/kg twice a day (maximum dose 13.8 - 40 g per day). For patients with fecal impaction, a bisacodyl suppository of 5 mg per day was used for 3 to 5 days.
Diagnosis of fecal impaction was conducted through abdominal examination, digital rectal examination, and, if necessary, simple abdominal radiography. Inclusion criteria included age 1 to 18 years, functional constipation diagnosed by a pediatric gastroenterologist based on the Rome IV criteria (14), and informed consent of the patient or parents to participate in the study. Patients with organic constipation and those taking medications that could alter bowel movements were excluded from the study.
In this study, the descriptive statistics section utilized mean and standard deviation to describe and report quantitative variables, while frequency and percentage were used for qualitative variables. In the analytical statistics section, demographic and basic characteristics were first compared between the two groups. An independent t-test was used to examine quantitative variables in the two groups. A chi-square test was used to compare qualitative variables in the two groups. To check the status of the response to the treatment at the investigated times, the frequency of recovery in the two groups was compared using the chi-square test.
Data analysis was conducted using SPSS version 20 software, and the significance level was considered less than 0.05 in all cases.
The Ethics Committee of the Hamadan University of Medical Sciences approved this study with the ethics code, the Deputy of Research and Technology IR.UMSHA.REC.1402.060.
4. Results
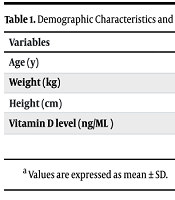
Of the 31 children with vitamin D deficiency, 10 (32.3%) were male, and of the 31 children without vitamin D deficiency, 12 (38.7%) were male (P > 0.05). There was no significant difference between the two groups in terms of demographic information (Table 1).
| Variables | Patients with Vitamin D Deficiency (N = 31) | Patients with Normal Vitamin D (N = 31) | P-Value |
|---|---|---|---|
| Age (y) | 6.1 ± 4.2 | 5.4 ± 3.5 | > 0.05 |
| Weight (kg) | 16.2 ± 5.8 | 14.7 ± 5.6 | > 0.05 |
| Height (cm) | 110.7 ± 4.2 | 111.3 ± 4.3 | > 0.05 |
| Vitamin D level (ng/ML ) | 15.96 ± 8.69 | 68.31 ± 17.11 | - |
Demographic Characteristics and Serum Vitamin D Levels of the Patients a
At the end of the second week of treatment, 45.2% of patients in the study group responded to constipation treatment, which was statistically significantly lower than the control group (74.2%) (P = 0.038). Additionally, at the end of the second week, the response to the treatment of constipation in patients with vitamin D deficiency with a serum level of 10 to 29 ng/mL (71.4%) was significantly better than in patients with vitamin D deficiency with a serum level of less than 10 ng/mL (20%) (P = 0.037).
At the end of the first month of treatment, 71% of patients in the study group and 90.3% of patients in the control group responded to constipation treatment, but this difference was not statistically significant (P = 0.108). Furthermore, at the end of the first month of treatment, in the group with vitamin D deficiency, 95.2% of patients with vitamin D levels between 10 and 29 ng/mL and 70% of patients with vitamin D levels less than 10 ng/mL responded to the treatment, with no statistically significant difference (P = 0.425). At the end of the second month of treatment, all patients in both groups responded to the treatment of constipation, and no significant difference was seen between the two groups.
5. Discussion
The results of this study showed that the response to constipation treatment at the end of the second week was significantly better in patients who were not vitamin D deficient. Additionally, the response to treatment was significantly better in patients whose serum vitamin D levels were 10 to 29 ng/mL compared to those whose serum vitamin D levels were less than 10 ng/mL. The relationship between vitamin D deficiency and intestinal motility disorders is not yet fully understood. Some believe that delayed small intestinal transit time may negatively affect the microbiota of the small intestine (15), or conversely, changes in the microbiota may initially affect the mucosal barrier and subsequently reduce intestinal motility due to microbial-derived metabolites (16).
Other studies have shown that vitamin D deficiency can increase susceptibility to gastrointestinal infections (17) and cause disruption of immune homeostasis (16, 18). The presence of vitamin D receptors on the surface of intestinal epithelial cells, lymphocytes, and macrophages suggests a possible relationship between vitamin D deficiency and the composition of the intestinal microbiota, which ultimately leads to the onset of several chronic diseases in the body (16, 19, 20).
Finally, some researchers hypothesize that intestinal motility disorder may be the initial trigger of an underlying autoimmune process in a specific genetic background, which manifests itself due to chronic vitamin D deficiency. This can cause metabolic/immunological damage to the epithelial and neuromuscular structures of the intestine. The damages that occur include increased intestinal permeability and bacterial translocation, with the degree and spread influenced by the severity of vitamin D deficiency (21-23). Few studies have been conducted to date on the prevalence of vitamin D deficiency in functional constipation, and no study was found in the literature on the effect of vitamin D deficiency on the treatment of constipation to compare with the present study.
A study by Panarese et al. on the prevalence of vitamin D deficiency in adult patients with chronic constipation showed that vitamin D levels were significantly lower in the functional constipation group than in the control group. Additionally, the prevalence of constipation symptoms was related to the severity of vitamin D deficiency (21). In another study by Metwally, conducted on 55 children with chronic functional constipation, vitamin D deficiency was significantly more common in constipated patients than in the control group (24).
Additionally, the results of Parker-Autry et al.'s study on women with fecal incontinence (31 cases) compared to healthy women (81 cases) showed that women with fecal incontinence had significantly lower vitamin D levels than the control group (25). The study conducted by El Amrousy et al. demonstrated that adolescent patients with IBS who received vitamin D supplementation experienced a significant improvement in clinical symptoms compared to the placebo group. Vitamin D supplementation in IBS patients can improve their symptoms and quality of life by reducing anxiety, stress, and depression (26).
5.1. Conclusions
The results of the present study showed that vitamin D deficiency has a negative effect on the response to constipation treatment in children with functional constipation. Therefore, it is advisable to check vitamin D levels in these patients and treat them if they are deficient.
